Mechanism of Disease & Patient Impact
Mike, a patient living with gMG. Mike has received compensation from Alexion Pharmaceuticals, Inc. and has a relative who works for Alexion.
Understanding pathophysiology, disease education, diagnosis, and treatment approaches
Generalized myasthenia gravis (gMG) is a rare autoimmune disorder that creates a fluctuating weakness of the voluntary muscles due to disrupted neuromuscular transmission. It is the most common type of myasthenia gravis (MG) and typically the most severe.1
A normal functioning complement system plays an important role in helping the body fight off infections. However, in gMG, the complement system attacks the area where the patient’s body sends signals to their muscles. This is known as impaired neuromuscular transmission, which can lead to weakness and fatigue of the muscles.1,2
Mechanism of Disease: In gMG, the complement cascade causes damage at the neuromuscular junction (NMJ)
WATCH: Understanding the Role of Complement in gMG
Learn more about the complement cascade
In gMG, the mechanisms that control the adaptive immune system do not function properly, as the adaptive immune system targets healthy tissues. With gMG, the pathology includes the generation of antibodies against acetylcholine receptors (AChRs). Anti-AChR antibodies disrupt signal transmission at the NMJ by blocking and reducing the number of functioning AChRs.3
- AChRs are found on the surface of muscle cells and are important for the generation of muscle contraction3
- On average, approximately 82% of patients with gMG are anti-AChR antibody positive4-8
At least three pathogenic mechanisms are believed to be responsible for disrupting the NMJ in anti-AChR antibody-positive gMG1,9:
- Complement-mediated postsynaptic membrane destruction
- Antigenic modulation
- Blockage of AChRs
Overview1,9,10: All three mechanisms are believed to be active in anti-AChR antibody-positive gMG, but complement-mediated postsynaptic membrane destruction could be a cause of functional AChR loss and consequent failure of neuromuscular transmission.
Anti-AChR antibody binding to AChRs activates the complement cascade, resulting in the downstream production of terminal complement components, including protein C5a (leading to inflammation) and C5b. C5b is the first protein included in the formation of the membrane attack complex (MAC) at the postsynaptic membrane.
MAC is composed of complement proteins C5b through C9 and damages the postsynaptic membrane and its associated structures, such as the membrane folds and dense clusters of AChRs. This causes a simplification and distortion of the postsynaptic membrane that reduces the overall number of AChRs.
Alteration of folds in the muscle membrane reduces the efficiency of neuromuscular transmission.
Healthy NMJ1,11,12
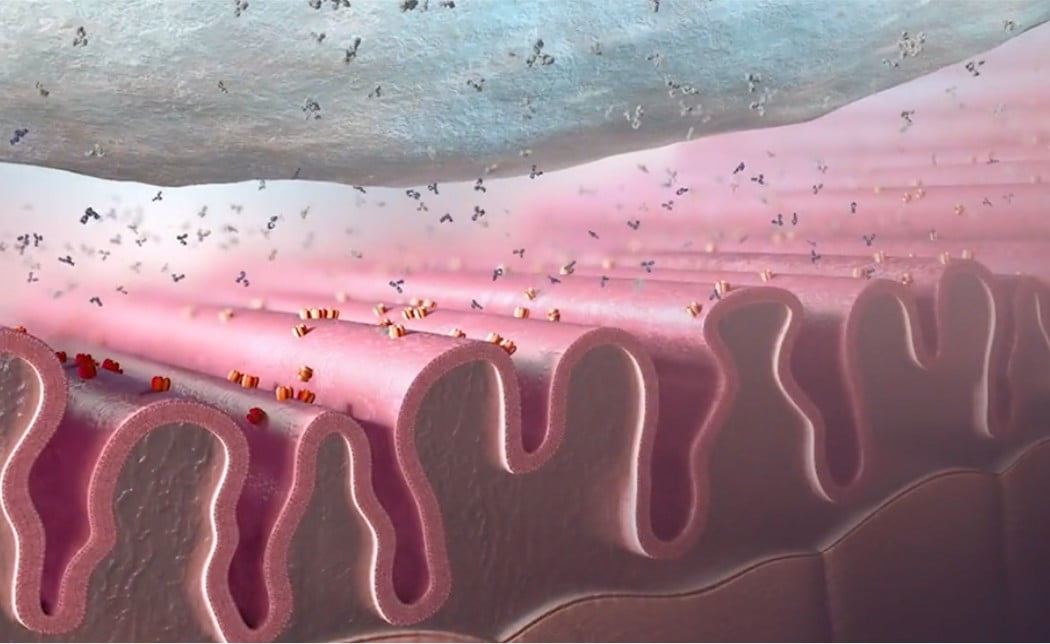

Typical folds in the muscle membrane
Complement
cascade leading to NMJ damage
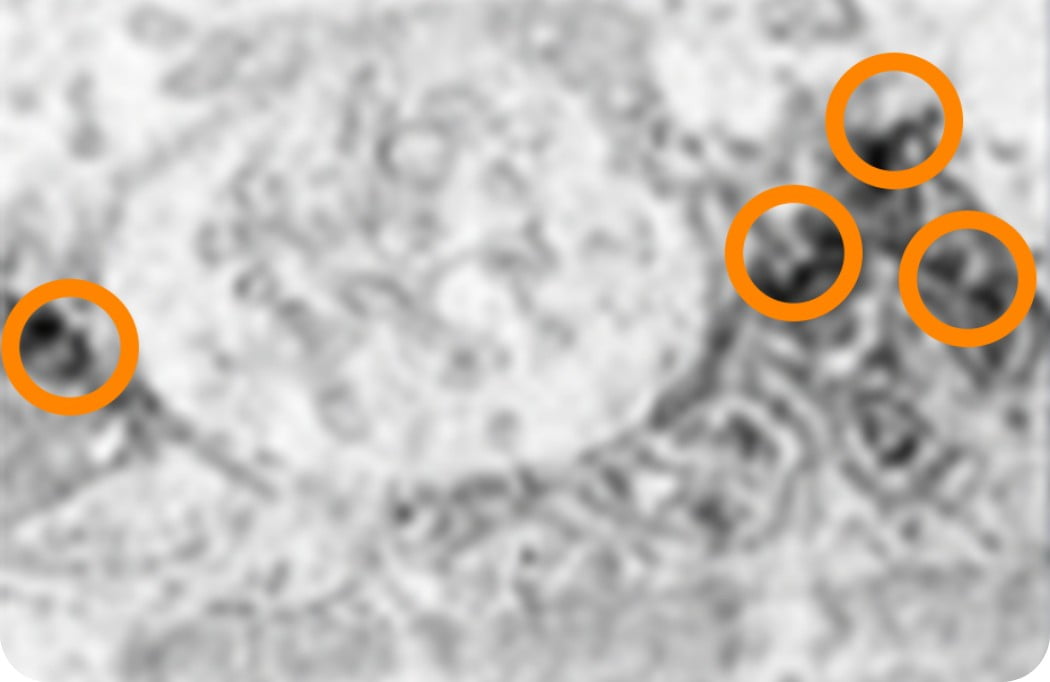
NMJ With Complement-Mediated Damage1,11,13
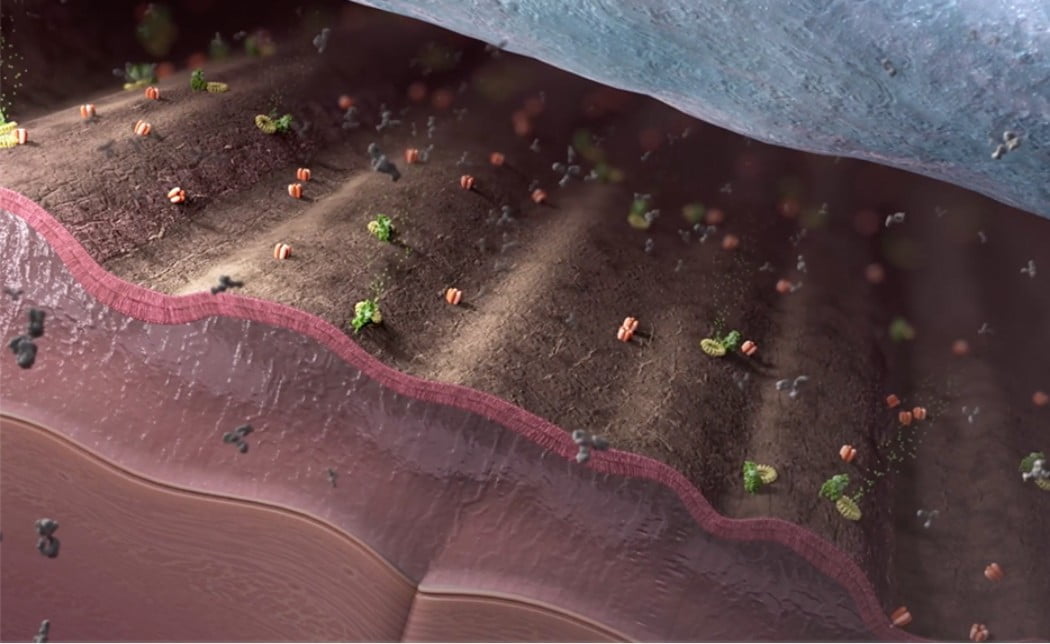
Simplified membrane morphology
Circled areas indicate deposition of C9 (MAC component).
Healthy NMJ image: Reprinted from Mayo Clin Proc, 52(5), Engel AG, et al. 267-280. © 2009, with permission from Elsevier.
NMJ With Complement-Mediated Damage image: Sahashi K, et al. J Neuropathol Exp Neurol. 1980;39(2):160-172. © 1980 by permission of Oxford University Press.
How gMG impacts patients
Prevalence of myasthenia gravis14,15:
Recent studies indicate that ~76% of diagnosed MG cases are generalized.
- Prevalence numbers may underestimate the true number of gMG cases, as the disease is underdiagnosed
- Generally prevalence is higher in females than in males, but reverses in older people; females often
have an
earlier age of onset compared to males
- The peak of incidence is between 20 and 40 years in females and between 60 and 80 years in males
Muscle damage caused by gMG can make daily activities and physical functions challenging
Some patients may struggle with16:
Vision
Breathing
Speech
Eating
Mobility
Common symptoms of gMG include11,17,18:
- Speech problems
- Difficulty chewing and swallowing
- Double vision/eyelid droop
- Altered facial expressions
- Difficulty holding one’s head up
- Trouble lifting the arms
- Weak grip
- Difficulty walking long distances or climbing stairs
- Trouble in rising from a sitting position
- Difficulty breathing
